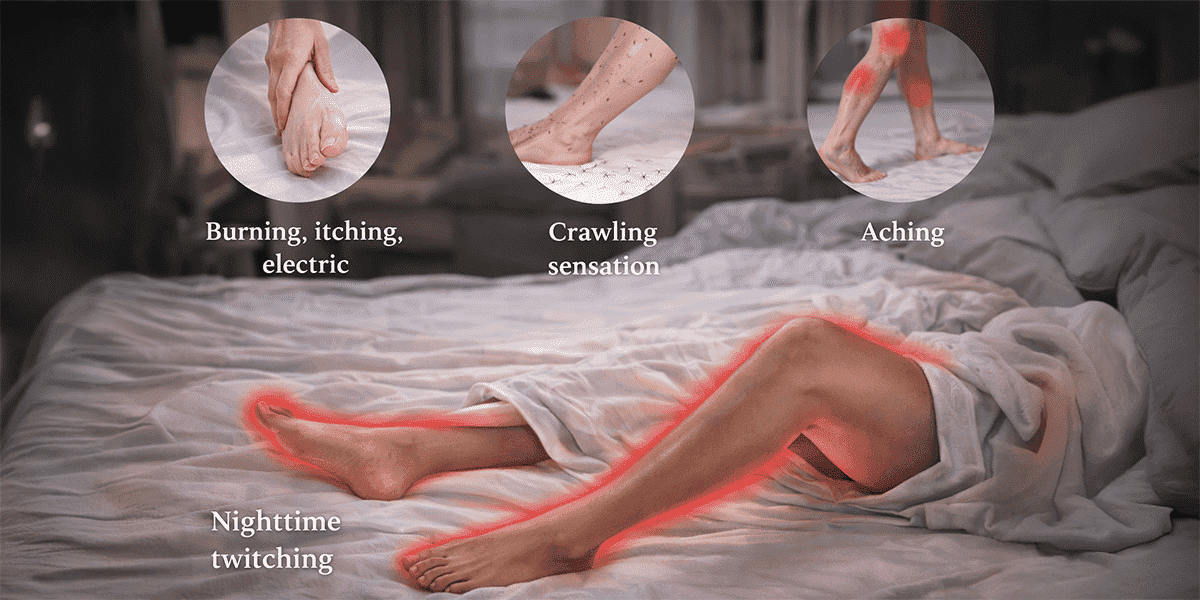
Many people dismiss night-time leg discomfort as a minor inconvenience. Yet for some, the urge to move the legs becomes a nightly struggle. A crawling, tingling, pulling, or electric sensation appears as soon as the body settles into rest. Relief comes only through movement, and sleep becomes repeatedly interrupted.
This pattern is consistent with Restless Legs Syndrome (RLS) a recognised neurological sensorimotor condition that commonly disrupts sleep and quality of life. A detailed clinical review in The Lancet Neurology describes RLS as a disorder associated with dopaminergic system dysfunction and altered iron regulation in the nervous system (Allen et al., 2014).
Sleep is not passive rest. During healthy sleep, the body typically downshifts: sympathetic nervous system activity reduces, blood pressure falls, and cardiovascular workload eases. When sleep is repeatedly fragmented, as may occur in moderate to severe RLS, this nightly regulation can become less stable over time.
Population-based research has identified associations between RLS and higher prevalence of hypertension and cardiovascular disease. Importantly, this is not the same as direct causation: RLS does not “cause” heart disease, but sustained sleep disruption and autonomic activation may contribute to long-term cardiovascular strain (Winkelman et al., 2011). The American Heart Association similarly notes that inadequate or poor-quality sleep is an important factor in cardiometabolic health risk.
In this context, addressing sleep quality is part of protecting cardiovascular health and long-term heart function.
Modern medicine recognises several contributors to RLS. Iron deficiency especially low ferritin is one of the most common reversible factors, and dopaminergic pathway dysfunction is central to symptom generation. RLS is also seen more frequently in association with chronic kidney disease, diabetes mellitus, pregnancy, peripheral neuropathy, and certain vitamin deficiencies.
Clinical practice guidelines recommend that in patients with restless legs syndrome and low ferritin (≤ 75 μg/L), clinicians should consider ferrous sulfate with vitamin C, and in moderate to severe cases, pharmacologic agents such as pramipexole or gabapentin enacarbil may be used to reduce symptoms (Winkelman et al., 2016).
Because several contributing factors are reversible, appropriate evaluation matters more than guesswork or self-treatment.
From an Ayurvedic perspective, symptoms resembling RLS are interpreted through disturbances in neuromuscular regulation and sleep rhythm often conceptualised through Vata imbalance and irregular daily routine. Rather than focusing only on the legs, classical approaches aim to restore rhythm, calm nervous system activity, and support circulation.
This view is not in conflict with modern science. Contemporary understanding recognises that sleep architecture and autonomic balance influence symptom severity and overall wellbeing.
For individuals seeking preventive lifestyle support in addition to medical evaluation, restoring daily rhythm and nervous system balance may be a useful focus.
Management begins with identifying contributors such as iron deficiency, vitamin B12 deficiency, renal impairment, and metabolic instability when relevant. Many people also benefit from regular moderate activity, consistent sleep timing, and reducing late-day triggers such as caffeine or alcohol.
In persistent or severe cases, neurological treatments including dopaminergic agents or other guideline-supported medications may be recommended under medical supervision, as reflected in the Neurology guideline summary (Silber et al., 2021).
If symptoms are recurring and sleep remains disrupted, a structured clinical consultation to assess sleep patterns, metabolic factors, and neurological contributors can help clarify the underlying drivers and guide an appropriate plan.
Professional assessment is advisable when leg restlessness occurs several nights per week, sleep is consistently disturbed, daytime fatigue becomes significant, or symptoms are worsening over time. Evaluation is also important when symptoms overlap with neuropathy, vascular conditions, or metabolic disorders, where the management pathway may differ.
Restless Legs Syndrome often begins quietly as discomfort that appears only when the body tries to rest. But when it becomes persistent, it can gradually erode sleep quality, and sleep is tightly linked to long-term neurological and cardiovascular regulation. The aim is not alarm. It is awareness: recurring symptoms deserve evaluation, especially when they disturb restorative sleep.
Allen RP, Picchietti DL, Garcia-Borreguero D, et al. (2014). Restless legs syndrome. [LINK]
Winkelman JW, et al. (2011). Associations of restless legs syndrome and cardiovascular disease in the US population. [LINK]
Winkelman, J.W., Armstrong 2016. Practice guideline summary: Treatment of restless legs syndrome in adults. [LINK]
American Heart Association. Sleep and Cardiovascular Disease. [LINK]
This article is provided for general health education and does not constitute medical advice, diagnosis, or treatment. Restless leg symptoms and sleep disturbances can have multiple causes and should be evaluated by a qualified healthcare professional, particularly if symptoms are frequent, worsening, or associated with fatigue, palpitations, or blood pressure concerns. Any supplements, medications, or therapeutic interventions should be used only under appropriate clinical guidance. Integrative and traditional approaches should complement not replace necessary medical evaluation and treatment.